


Recognition of andropausic symptoms
- *Corresponding Author:
- Dr J Mailhot
3030, boul du Carrefour, suite 305, Laval, Quebec H7T 2P5
Tel: 450-686-1737
Keywords
Cognitive function; Masculinity; Mood disorders; Nervous symptoms; Sexuality; Vasomotor symptoms; Virility
Climacteric symptoms in women, as well as the term ‘menopause’, are well recognized y the medical community. Menopause relates to a patient’s clinical status and is confirmed by a biological test. The aging phenomenon in men is the result of a process that is different from that in women; however, the clinical manifestations may be similar. The term ‘andropause’ is used to define a partial testosterone deficiency in the aging male. Although the term is basically a misnomer, its use has been accepted by both health professionnals and lay people. Attempts to find a more accurate term, such as andropenia, testopenia, partial androgen deficiency in the aging male, androgen deficiency in aging males, aging male’s symptoms (AMS) and male menopause, have proved to be unsuccessful.
Definition
Andropause is a clinical entity that is related to aging. It is not a disease, but rather, a slow physiological process that is secondary to decreases in multihormonal concentration, multihormonal production and multihormonal efficacy, and a decreased capacity of receptors to respond to stimuli. The hormones testosterone, luteinizing hormone, follicle-stimulating hormone, growth hormone, dehydroepiandrosterone), (dehydroepiandrosterone sulfate), androstenedione, melatonin and estradiol have been studied.
Screening for Andropause
Morley’s questionnaire [2] is the only known and validated questionnaire that is used as a screening test for andropause. If the test result is negative, andropause can be ruled out as a diagnosis. For the test to be positive, a male patient must answer ‘yes’ to question 1 or 7, or to any other three questions (Table 1).
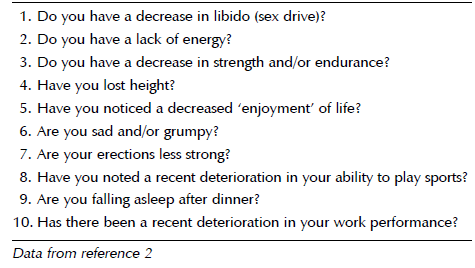
Table 1: Morley’s screening questionnaire for andropause
After the questionnaire (the first step toward diagnosing andropause) is completed, it is necessary to follow good clinical practice guidelines by completing a clinical evaluation, ruling out any other disease with similar symptoms and confirming the diagnosis by a specific laboratory test (the latter is discussed by Dr Brisson on pages 78 to 80 in the present issue).
Clinical Diagnosis of Andropause
The symptoms of andropause can be related to testosterone target organ (brain, skin, muscle, liver, synovial tissue, kidney, male sex organs, bone marrow and bone) deficiencies; however, has this correlation proven to be true or reliable? Suggested answers in published articles are regularly confirmed by recent research conclusions, but the final and most accurate answer to the above question awaits future research findings.
In 1998, the Canadian Andropause Society published practice recommendations for screening, monitoring and treating men affected by andropause [3]. The recommendations included a list of symptoms that are classified into four areas of investigation. In 1999, Heinemann et al [4] suggested a new AMS rating scale. The scale was translated into French and adapted by Drs P Alarie and R Villeneuve; it is undergoing validation. In 2001, Heinemann et al [5] published the results of the validation process for the English version of the AMS questionnaire.
In the questionnaires and list of symptoms of andropause listed above, gonadal decline-related clinical manifestations remain fairly constant [6-9]. However, Dobs et al [10] found that men with idiopathic low testosterone, compared with men with a pituitary tumour, complained more of impotence, erectile dysfunction and depression.
Symptoms of Andropause
As noted by McKinley [11], because aging is a multifactorial phenomenon, a multidisciplinary management approach to andropause is required and is richly rewarding. In a workshop on andropause [12], the Quebec Task Force on Andropause outlined the following aspects that physicians must keep in mind when evaluating and trying to understand andropause.
• Andropause symptoms may be present with or without erectile dysfunction.
• Symptoms are usually progressive.
• There is wide inter- and intravariation of symptoms in men.
• Self-perception of andropause symptoms is influenced by a patient’s basal health status.
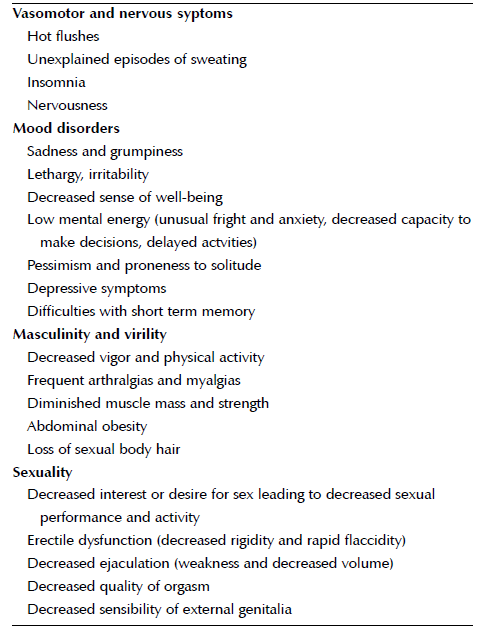
Based on the author’s experience and the experience of clinicians involved in the management of andropause, the three most frequent sypmtoms of andropause are hot flushes, decreased global well-being and decreased sexual desire. The numerous clinical manifestations are mostly testopenic symptoms that can be classified according to several areas of investigation (Table 2).
Excluding erectile dysfunction, the similarity of aging symptoms in men and women has been recognized for over 50 years. However, as stated by Heinemann et al [13], women report more symptoms than men, men mention symptoms only if they are specifically asked about them, and the perception of symptoms by men and women changes with sex and age.
Conclusion
Andropause is a clinical entity. The symptoms of andropause are numerous, and are related to decreased multihormonal concentration and efficacy. To date, testosterone deficiency seems to be a significant factor in the male aging process. The clinical diagnosis of andropause combines the art of medicine with the thoroughness of scientific rigour. Time will bring the evidence-based medicine.
References
- Hesch RD. The health of the aging person. Aging Male 1999;2:129-30.
- Morley JE, Charlton E, Patrick P, et al. Validation of a screening questionnaire for Androgen Deficiency in Aging Males (ADAM). Proceedings of the Endocrine Society. Toronto, 1998:136
- Tremblay RR, Morales A. Canadian practice recommendations for screening, monitoring and treating men affected by andropause or partial androgen deficiency. Aging Male 1998;1:213-8.
- Heinemenn LAJ, Zimmerman T, Vermeulen A, Thiel C, Hummel W. A new ‘aging male’s symptoms’ rating scale. Aging Male 1999;2:105-14.
- Heinemann LAJ, Saad F, Thiele K, Wood-Dauphinee S. The Aging Male’s Symptoms rating scale: Cultural and linguistic validation into English. Aging Male 2001;4:14-22.
- Nicopoulou SC, Adamopoulos DA. Gonadal decline-related manifestations in aging hospital doctors. Aging Male 2001;4:8-13.
- Tenover JL. Testosterone and the aging male. J Androl 1997;18:103-6.
- Morales A. Andropause, a misnomer for a true clinical entity. 7th International Congress of Andrology. Montreal, June 2001.
- Vermeulen A. The male climacterium. Ann Med 1993;25:531-4.
- Dobs AS, El-Dery S, Wand G, Wiederkehr M, Bell DSH, Mayo MS. Central hypgonadism: Distinguishing idiopathic low testosterone from pituitary tumors. Endocr Pract 1998;4:355-9.
- McKinley JB. So you want to study male aging and health? Ten questions in search of an answer. 2nd International Congress on The Aging Male. Geneva, February 9 to 13, 2000.
- Mailhot J, Tremblay RR, Brisson G. Quebec Task Force on Andropause. Workshop on Andropause. Montreal, May 2, 1998.
- Heinemann LAJ, Thiele C, Assmann A, Zimmerman T, Hummel W, Vermeulen A. Sex differences in ‘climacteric symptoms’ with increasing age? A hypothesis-generating analysis of cross-sectional population surveys. Aging Male 2000;3:124-31.
- *Corresponding Author:
- Dr J Mailhot
3030, boul du Carrefour, suite 305, Laval, Quebec H7T 2P5
Tel: 450-686-1737
Abstract
The aging phenomenon in men is the result of a process that is different from that in women; however, the clinical manifestations may be similar. The term ‘andropause’ is used to define partial testosterone deficiency in the aging male. The symptoms of andropause are numerous, and are related to decreased multihormonal concentration and efficacy. To date, testosterone deficiency seems to be a significant factor in the male aging process. The present paper reviews screening, diagnosis and the symptoms of andropause.
-Keywords
Cognitive function; Masculinity; Mood disorders; Nervous symptoms; Sexuality; Vasomotor symptoms; Virility
Climacteric symptoms in women, as well as the term ‘menopause’, are well recognized y the medical community. Menopause relates to a patient’s clinical status and is confirmed by a biological test. The aging phenomenon in men is the result of a process that is different from that in women; however, the clinical manifestations may be similar. The term ‘andropause’ is used to define a partial testosterone deficiency in the aging male. Although the term is basically a misnomer, its use has been accepted by both health professionnals and lay people. Attempts to find a more accurate term, such as andropenia, testopenia, partial androgen deficiency in the aging male, androgen deficiency in aging males, aging male’s symptoms (AMS) and male menopause, have proved to be unsuccessful.
Definition
Andropause is a clinical entity that is related to aging. It is not a disease, but rather, a slow physiological process that is secondary to decreases in multihormonal concentration, multihormonal production and multihormonal efficacy, and a decreased capacity of receptors to respond to stimuli. The hormones testosterone, luteinizing hormone, follicle-stimulating hormone, growth hormone, dehydroepiandrosterone), (dehydroepiandrosterone sulfate), androstenedione, melatonin and estradiol have been studied.
Screening for Andropause
Morley’s questionnaire [2] is the only known and validated questionnaire that is used as a screening test for andropause. If the test result is negative, andropause can be ruled out as a diagnosis. For the test to be positive, a male patient must answer ‘yes’ to question 1 or 7, or to any other three questions (Table 1).
Table 1: Morley’s screening questionnaire for andropause
After the questionnaire (the first step toward diagnosing andropause) is completed, it is necessary to follow good clinical practice guidelines by completing a clinical evaluation, ruling out any other disease with similar symptoms and confirming the diagnosis by a specific laboratory test (the latter is discussed by Dr Brisson on pages 78 to 80 in the present issue).
Clinical Diagnosis of Andropause
The symptoms of andropause can be related to testosterone target organ (brain, skin, muscle, liver, synovial tissue, kidney, male sex organs, bone marrow and bone) deficiencies; however, has this correlation proven to be true or reliable? Suggested answers in published articles are regularly confirmed by recent research conclusions, but the final and most accurate answer to the above question awaits future research findings.
In 1998, the Canadian Andropause Society published practice recommendations for screening, monitoring and treating men affected by andropause [3]. The recommendations included a list of symptoms that are classified into four areas of investigation. In 1999, Heinemann et al [4] suggested a new AMS rating scale. The scale was translated into French and adapted by Drs P Alarie and R Villeneuve; it is undergoing validation. In 2001, Heinemann et al [5] published the results of the validation process for the English version of the AMS questionnaire.
In the questionnaires and list of symptoms of andropause listed above, gonadal decline-related clinical manifestations remain fairly constant [6-9]. However, Dobs et al [10] found that men with idiopathic low testosterone, compared with men with a pituitary tumour, complained more of impotence, erectile dysfunction and depression.
Symptoms of Andropause
As noted by McKinley [11], because aging is a multifactorial phenomenon, a multidisciplinary management approach to andropause is required and is richly rewarding. In a workshop on andropause [12], the Quebec Task Force on Andropause outlined the following aspects that physicians must keep in mind when evaluating and trying to understand andropause.
• Andropause symptoms may be present with or without erectile dysfunction.
• Symptoms are usually progressive.
• There is wide inter- and intravariation of symptoms in men.
• Self-perception of andropause symptoms is influenced by a patient’s basal health status.
Based on the author’s experience and the experience of clinicians involved in the management of andropause, the three most frequent sypmtoms of andropause are hot flushes, decreased global well-being and decreased sexual desire. The numerous clinical manifestations are mostly testopenic symptoms that can be classified according to several areas of investigation (Table 2).
Excluding erectile dysfunction, the similarity of aging symptoms in men and women has been recognized for over 50 years. However, as stated by Heinemann et al [13], women report more symptoms than men, men mention symptoms only if they are specifically asked about them, and the perception of symptoms by men and women changes with sex and age.
Conclusion
Andropause is a clinical entity. The symptoms of andropause are numerous, and are related to decreased multihormonal concentration and efficacy. To date, testosterone deficiency seems to be a significant factor in the male aging process. The clinical diagnosis of andropause combines the art of medicine with the thoroughness of scientific rigour. Time will bring the evidence-based medicine.
References
- Hesch RD. The health of the aging person. Aging Male 1999;2:129-30.
- Morley JE, Charlton E, Patrick P, et al. Validation of a screening questionnaire for Androgen Deficiency in Aging Males (ADAM). Proceedings of the Endocrine Society. Toronto, 1998:136
- Tremblay RR, Morales A. Canadian practice recommendations for screening, monitoring and treating men affected by andropause or partial androgen deficiency. Aging Male 1998;1:213-8.
- Heinemenn LAJ, Zimmerman T, Vermeulen A, Thiel C, Hummel W. A new ‘aging male’s symptoms’ rating scale. Aging Male 1999;2:105-14.
- Heinemann LAJ, Saad F, Thiele K, Wood-Dauphinee S. The Aging Male’s Symptoms rating scale: Cultural and linguistic validation into English. Aging Male 2001;4:14-22.
- Nicopoulou SC, Adamopoulos DA. Gonadal decline-related manifestations in aging hospital doctors. Aging Male 2001;4:8-13.
- Tenover JL. Testosterone and the aging male. J Androl 1997;18:103-6.
- Morales A. Andropause, a misnomer for a true clinical entity. 7th International Congress of Andrology. Montreal, June 2001.
- Vermeulen A. The male climacterium. Ann Med 1993;25:531-4.
- Dobs AS, El-Dery S, Wand G, Wiederkehr M, Bell DSH, Mayo MS. Central hypgonadism: Distinguishing idiopathic low testosterone from pituitary tumors. Endocr Pract 1998;4:355-9.
- McKinley JB. So you want to study male aging and health? Ten questions in search of an answer. 2nd International Congress on The Aging Male. Geneva, February 9 to 13, 2000.
- Mailhot J, Tremblay RR, Brisson G. Quebec Task Force on Andropause. Workshop on Andropause. Montreal, May 2, 1998.
- Heinemann LAJ, Thiele C, Assmann A, Zimmerman T, Hummel W, Vermeulen A. Sex differences in ‘climacteric symptoms’ with increasing age? A hypothesis-generating analysis of cross-sectional population surveys. Aging Male 2000;3:124-31.
